
Written by Lauren Chin
Mention being a doctor, and you often see people’s eyes widen with notions of success, being rich, and reaching the pinnacle of the social and occupational pyramid. However, the reality of being a physician is far from rosy: even medical doctors face their own social inequities within their profession.

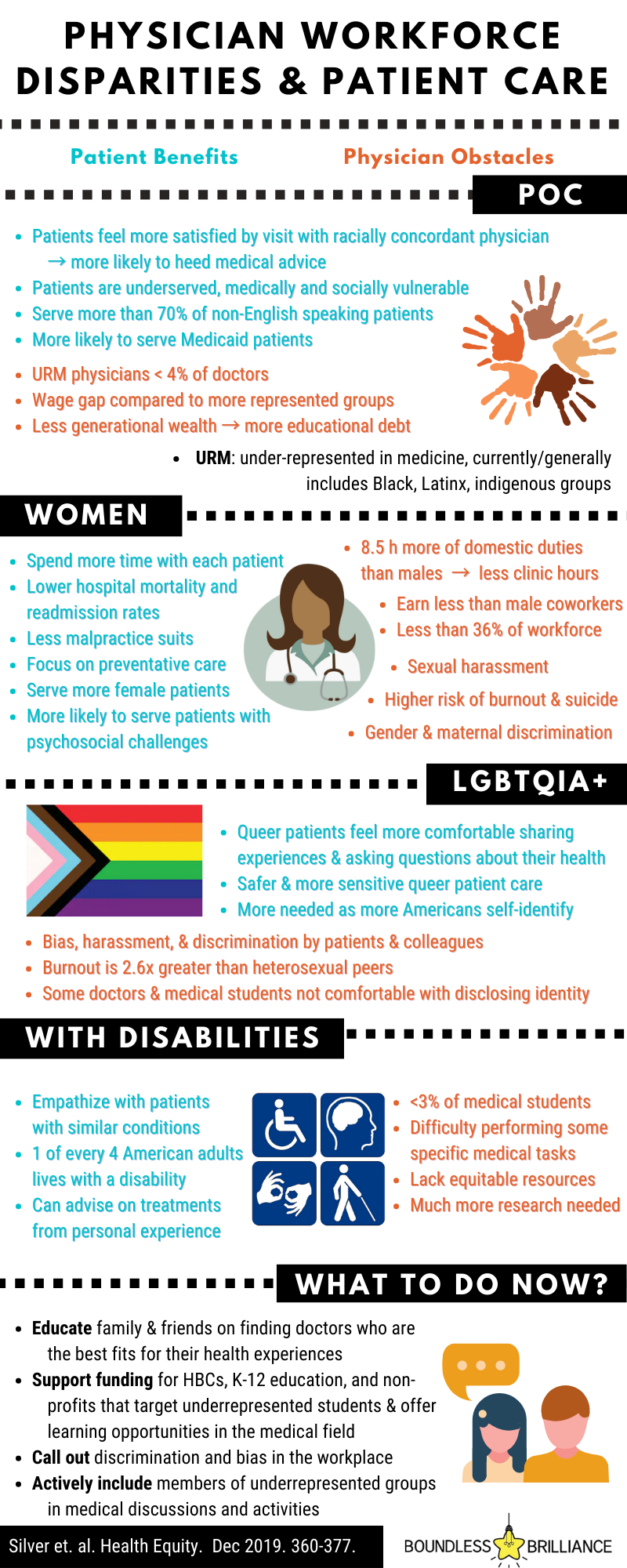
Medical researchers and doctors (Silver, Bean, Slocum, et al.) recently looked at hundreds of articles containing discussions centered around women, racial and ethnic minorities, individuals with disabilities, and sexual and gender minorities who currently work as physicians in the United States in order to investigate how workforce disparities impact these groups, and if these disparities affect patient care as well. The conclusion is unfortunate: inequities within physician work culture warrant a public health issue that both harms physicians’ own health and compounds already known patient disparities within the American healthcare system.

Such challenges to underrepresented physicians can lead to physician burnout (physical or emotional exhaustion from chronic workplace stress and reduced sense of accomplishment or personal identity) and harm overall patient care even more. However, locating these gaps in the medical doctor workforce does offer us an opportunity to initiate programs and support to uplift those groups feeling the brunt of these disparities.

Women Physicians
Women made up only 35% of the active physician workforce in 2017. However, female physicians are more likely to emphasize preventative care and counseling and see female patients and patients with psychosocial issues (e.g., depression) as compared to their male counterparts.
Research even shows female hospitalists’ mortality and readmission rates are lower. Spending more time with each patient is characteristic of female physicians, but comes at the cost of having to work longer hours to see equal amounts of patients as male physicians, as well as complete an average 8.5 hours more than their male colleagues dedicated to family and household commitments.
Sadly, instances of gender discrimination and sexual harassment during practice or medical school also contribute to greater job stress, worse performance, and sometimes even withdrawal from the field completely. Altogether, burnout for women physicians is estimated to be much higher than for male physicians, and in some specialties such as primary-care, twice as likely as men. These strains in work-life balance and emotional exhaustion often lead to women physicians cutting their clinical hours and ultimately reducing the overall benefits that the patient population receives from them.

Because of greater challenges in work-life balance and work stressors, female physicians are more likely to experience burnout and are nearly twice as likely to die by suicide as male physicians—on top of the already shocking statistic that almost one physician dies by suicide each day. Furthermore, work-life inequities such as pay gaps exist even when factors such as specialty, work hours, experience, and ethnicity have been normalized. The increased debt that results from this already harrowing experience, along with inequitable promotions in academic and clinical medicine, contributes to higher emotional exhaustion in women than men.

Racial and Ethnic Minority Physicians
The Association of American Medical Colleges (AAMC) currently refers to physicians of (but not limited to) Black, Latinx, and Indigenous heritage as URM: underrepresented in medicine. This term is, however, flexible in the groups that it encompasses to account for future progress. For example, Hispanic and Black physicians made up only 4% of the workforce in 2014, but the two groups make up more than a quarter of the U.S. population combined. URM physicians serve an astounding majority of minority patients and over 70% of non-English speaking patients, making them a critical component of the U.S. healthcare system.
Having a physician who understands a patient’s culture can increase the likelihood of that patient disclosing their daily habits or traditions, such as their diet, that may be relevant to their preventative care or treatment and personalize their health experience. However, current workforce representation is not the only thing that is low; URM matriculation from medical schools barely hits the teens in percentages, which poses projected challenges in physician demand as the national population of these groups is expected to increase along with increased medical insurance access.

In some studies, URM physicians have reported higher career satisfaction and lower perceived stress than white peers, perhaps due to resiliency in their more challenging paths to becoming physicians; they also tend to feel a greater sense of community responsibility in working with vulnerable and low socioeconomic status patients. On the patient side, many patients have expressed preference for racially similar physicians, citing more satisfaction after visits and more adherence to health recommendations preventative services.
However, taking care of minority patients may be a double-edged sword: because patients are likely to be from underserved and more medically and socially vulnerable populations, and thus present with more complex medical and psychosocial conditions while also experiencing greater environmental and structural challenges, URM physicians have to essentially jump through more hoops to provide high-quality care and reach job satisfaction. Additionally, URM physicians have been shown to receive less compensation; when compounded with less generational wealth and greater educational debt, these individuals are at a large disadvantage when practicing compared to more represented ethnic and racial groups after becoming a physician. This may lead to burnout or decreased working hours, further exacerbating healthcare disparities that affect minorities.

Physicians With Disabilities
Information on physicians with disabilities still remains scarce, though a 2005 report suggested that 2-10% of practicing physicians lived with a disability, an impairment such as, but not limited to, those of hearing, vision, mobility, and cognition that limits easy participation in certain activities. While disabilities may make some parts of becoming and practicing as a physician challenging, it is very valuable for patients to receive care from physicians who can accurately empathize with their experiences or advise on often overlooked details of procedures or regimens, such as pain or the feasibility of taking multiple pills a day, that physicians who do not live with a certain disability may not know. This is especially important considering that a quarter of the American adult population lives with some type of disability.
In medical schools, less than 3% of matriculated students reported a disability such as ADHD or chronic health issues (sometimes referred to as “invisible disabilities”), or more “visible” disabilities such as those of mobility. Because of the lack of information on physicians and medical students with disabilities, more research must be done in order to learn how to meet these individuals’ additional needs, optimally support them, and emphasize their benefits and strengths to the health community.

Queer Physicians
Because LGBTQ+ patients have historically been at greater risk for some health issues such as anxiety, HIV/AIDS, and negative side effects of long-term hormone therapy, it is extremely important that patients can rely on health providers that understand their experiences firsthand and who can provide them safe and sensitive care. For example, queer minor patients who are not yet “out” to their family may face heightened anxiety about their doctor’s reaction to their identity or fear that their doctor may inadvertently disclose this information to their parents. One current challenge that we face in determining the true impact and experiences of queer physicians and patients is that individuals may not feel comfortable with disclosing that part of their identity due to personal circumstances, resulting in a lack of data. However, we can be sure that as more Americans self-identify as LGBTQ+, there will be an increasing need for queer-competent physicians.
Patient bias also plays a role in increased stress for queer health providers; one study found that 30% of patients wanted to switch providers when they found out that their doctor was gay or worked in a clinic with openly LGBTQ+ physicians. Queer medical students have been found to be more than twice as likely to report burnout and depression than heterosexual peers, and physicians unfortunately also have to face and witness LGBTQ+ harassment in their workplaces, adding further stress to an already arduous occupation.

So what can we do as a society?
The U.S. healthcare system is full of inequities in care, but diversity, representation, and inclusion in the medical field can help close these gaps. First, we can start off by supporting more research on physicians in these aforementioned communities, especially with regard to the experiences of doctors and medical students who are queer, have disabilities, or have intersectional identities, where current research is most lacking. In the workplace, interventions such as well-being programs, gender-inclusive restrooms, personal implicit bias tests, emphasizing career-long learning of cultural competency, and creating actively inclusive climates for all identities provide great starting points for healthcare institutions to fight bias and burnout in their workforce. In academia, actions such as blind grant applications, free or reduced medical school tuition, LGBTQ+-inclusive educational materials, and even increasing K-12 education funding can all have benefits in eliminating barriers for underrepresented groups in medicine. Overall actions to educate patients and the general U.S. population, including our own friends and family, that doctors from these groups are just as educated and experienced as those from more represented groups in medicine is also extremely important, as is supporting individuals in finding the best physician for each of them personally.

While medical programs are now seeking to accept more diverse applicants and support their students, it is critical to not only accept larger amounts of minority applicants to medical programs and institutions, but to also ensure that minority applicants compose a larger proportion of the applicant pool to begin with--so much so that we may never have to use the term “underrepresented” again. This entails garnering interest in medicine in individuals from these underrepresented groups early on and supporting them through their journey, which is where programs like Boundless Brilliance come in. By encouraging children with these underrepresented identities to pursue roles in medicine, as well as other positions in the STEM workforce, and providing them resources to learn more about basic STEM skills and opportunities, we help to remove the initial barriers that have discouraged people in the past from viewing themselves as future physicians. This not only helps diversify the field of medicine but also strengthens the possibility for the groups these budding physicians represent to receive the optimal care they deserve in the not-so-distant future.
Looking for more resources to empower and inspire your young scientist? Check out our workbook full of exciting science experiments and empowering activities!
Learn more and purchase today!
